As America’s opiate epidemic rages on, calls for “treatment not punishment” dominate the national media. The hypocrisy of this response is not lost on a range of commentators: the reported move away from criminalization, they argue, is yet another example of racist drug policy. White people get treatment and poor people of color get punishment. Again.
A cursory reading of national media seems to confirm this long-standing narrative of White, middle-class drug users as victims, not criminals. For example, the New York Times’ coverage of suburban drug users has invited sympathy and identification with the people in the stories, encouraging the reader to see themselves, their child, or someone they know in the stories of good people raised in loving families who became opiate addicts almost by accident. The accompanying pictures to these articles show white people hugging as they leave drug treatment and well-dressed parents looking at pictures of the son or daughter they’ve lost to heroin. Photos of attractive and smiling teenagers—someone’s children—remind us of the promise and potential extinguished by an overdose. And yet, the Times is also savvy enough to contextualize this new drug panic when they write, “In Heroin Crisis, White Families Seek Gentler War on Drugs” (Oct. 30, 2015). They subtly remind the reader that non-White addicts get punishment and harshness when they refer to the White opiate crisis as a “new era” characterized by “striking shifts… some local police departments have stopped punishing many heroin users.” It is only because the users are White that a redemptive narrative of families and police coming together to stop opiate use can gain traction in print and in legislative bodies.
And yet, this same media inadvertently invites a disruption to the dominant reading. In regional coverage of the opiate panic in Vermont, for example, the “crisis” of opiate use is framed as a “scourge” in quaint Bennington and in Rutland, a “blue-collar” town filled with addicts and drug dealers. The images accompanying these stories show a different tale of White drug use. Stephanie Predel, with dark circles under her eyes, is smoking a cigarette (itself a symbol of disrepute) in front of a ramshackle and dirty house. Alfred Hickey, looking tired and disheveled, is captioned to cast doubt: “[he] said he quit heroin.” Twenty-year-old Hailey Clark, here depicted as someone’s mother rather than daughter, is crying after losing custody of her son because of a heroin conviction. And two state troopers are pictured searching a suspect’s car for drugs. The story of opiates in Vermont is the opposite of innocence and community cohesion. As in suburban America, opiates are the culprit, but the response is markedly different. Poor White drug users get punishment.
While media coverage hints at this differential treatment among White users, an almost exclusive focus on racial inequality in drug policy has been repeated without question by both drug policy reformers and scholars. For good reason, many are ready to see yet another example of racism in current drug policy: drug scares have a deeply racist history. The “crack epidemic” of the 1980s is a stark example of the way the fear of drugs was used to justify increased criminalized repression of people of color. The egregious sentencing disparity between crack (coded as a Black drug) and powder cocaine (coded as a White drug), emerged through bi-partisan Congressional consensus. Sentencing disparities by race remain a hallmark of the War on Drugs. The first drug scares in the U.S., which were also about opiates, were reflections of thinly veiled anti-Chinese racism in the late 19th and early 20th centuries. Drug prohibition often relies on the image of a demonized racial other whose drug use threatens social stability.
But if we see only racial animus in drug scares, we overlook another engine of social control and harm: classism. The primary framing of the opiate epidemic as “White and middle-class” and the assumption that all White drug users have privilege serves to obscure the ways in which class figures prominently as a dividing line between which drug users are subjected to and exempted from punitive social control.
For the past several years, I have studied the opiate panic in Vermont. I’ve lived in the town often referred to as “the heroin capital of New England”, talking with drug users, addiction medicine doctors, prosecutors, judges, defense attorneys, police and probation officers, jail superintendents, harm reduction providers, and community members, many of them neighbors. The notion that this is a “gentler drug war” conflicts with the punitive response I see in practice, in which poor White drug users are caught at the intersection of the criminal justice, drug treatment, and child protection systems.
Pennsylvania’s governor, Tom Wolf, announces an expansion of a program to equip DCNR rangers with naloxone to reverse opioid overdoses. Governor Tom Wolf, Flickr CC
Pervasive Criminalization
Something as simple as taking the bus to work, an hour and a half commute, turns into a lesson about life at the margins in a state governed by an opiate panic. Conversation inevitably turns to why someone is riding public transportation in a rural area where a vehicle is a necessity. I hear stories of people whose cars have been seized by the police, through asset forfeiture, returned to them so damaged from drug searches that the cars are beyond repair. People travel two hours south or north to meet with probation officers; an appointment in the afternoon means they might have to take the day off from work, spending several hours loitering in a local park or library until they can check in for the weekly supervision that costs them $100 a month. Lapses in regular ridership are often explained by a return to jail because of missed appointments with probation officers or positive drug tests.
Poor White people are caught up in the system of punitive and medical control that relies heavily on the criminal justice system and its extension, compulsory drug treatment. People who came into the syringe exchange where I volunteered would complain that there were police officers waiting at the door to the methadone clinic around the corner. When I asked a clinic administrator about the cops, she reminded me that you can’t trust “these people… remember why they’re here.” And though she acknowledged that the clinic was providing a social service to sick people, it didn’t change the fact that many of their patients were also criminals. Law enforcement and social workers decide together how to respond to a “dirty urine” report from drug treatment (weekend stints in jail are a common consequence). On a recent trip to a county correctional facility, the superintendent told me that about 80% of the inmates were there for drug or drug-related charges. We pass through a dark hallway: as my eyes adjust, I see a figure in a cot in a small, unlit cell. This is the “medically managed detox”: I see three guards watching the man, but I am told a doctor is in the facility. For many rural drug users, the first “medical care” they receive is in jail.
Many addicts began with legitimate prescriptions for pain medications, like Dilaudid, and turned to street drugs when their prescriptions were cut off. The.Comedian, Flickr CC
Punitive Medicalization
Much of the media focus on the opiate panic in Vermont has centered on the willingness of the former governor, Peter Shumlin, to tackle the panic head-on by referring to it in his 2015 State of the State address. And Vermont is praised for its efforts to get drug users, especially those with criminal convictions, into “medically assisted treatment” (opiate replacement therapy such as methadone or buprenorphine) quickly. The reality for the drug users I’ve spoken with is that this approach, praised by many treatment providers and advocates across the country as an “enlightened” way to treat opiate addiction, becomes another form of control.
“Heroin or nothing,” as Steven, a man I met at the syringe exchange, put it. Those were his options. He’d broken his back several years before, and opiates helped with the lasting pain as he continued in manual labor, working odd jobs and moving furniture. But treating the physical pain now meant dealing with the “pain in the ass” of the system, of the methadone treatment providers and probation officers. Steven was among the many people I encountered who had initially started using legally obtained opiates to treat pain from work-related injuries, only to find their access limited by increasingly stringent state prescribing regulations. People like Steven turned to heroin not because they preferred it, but because they could no longer get prescription painkillers. The problem is made even worse by the push of some states to ban alternatives to opiates, like kratom, which are often sold online and in stores. Kratom has been hailed by those formerly dependent on painkillers for its ability to make withdrawal easier to deal with, and helps users get back on their feet. But, with some states like Wisconsin and Indiana banning kratom (mitragyna speciosa) capsules, it makes it difficult for users to source alternatives.
Conversations with addiction medicine providers echo the judgment about which some of the drug users I’ve spoken with complain. In the New York Times’ coverage of the suburban opiate panic, doctors identify with their patients, perhaps even knowing them socially. This is not the case in Vermont, where the class divide between doctors and patients is wide. Even the most sympathetic physicians I spoke with endorsed monitoring and coerced treatment. One said that there was “no high-level thinking in Vermont” and “no one understands the medical piece.” When I asked about the best way to treat addiction, this doctor told me it was suboxone (buprenorphine) combined with “tight control… put an ankle bracelet on them and tightly monitor them… If you mess up, you go to jail. Folks do best when there are consequences.” Other medical providers were frustrated with their patients, viewing their poverty-related struggles such as lack of transportation or difficulty finding employment as “excuses” for not succeeding in recovery. Their patients’ continued smoking and poor eating habits are also a regular source of frustration. One doctor who called addiction a “disease” insists that the criminal justice oversight of a sick person is not a contradiction, but a mechanism to ensure sorely needed “accountability.”
In my book Judging Addicts, I detailed the merger of the medical and punitive frameworks of addiction and how they’ve come to characterize the modern treatment system in the U.S.: criminalization and medicalization are complementary, rather than contradictory approaches, I argued. This merger is apparent in Vermont where the treatment and punishment systems are deeply intertwined. And yet, this mingling has not necessarily led law enforcement to a more progressive or lenient view of addicts or for medical providers to argue that addicts shouldn’t be criminally punished. A prosecutor who was assigned to a drug court told me: “Their problem isn’t really addiction, their problem is that they’re criminals. And their parents were criminals.” This person was reluctant to accept the narrative that these people were sick even though she was working as part of a Drug Court Team whose ostensible goal was to get addicts the services they need to become drug and alcohol, and thus crime, free.
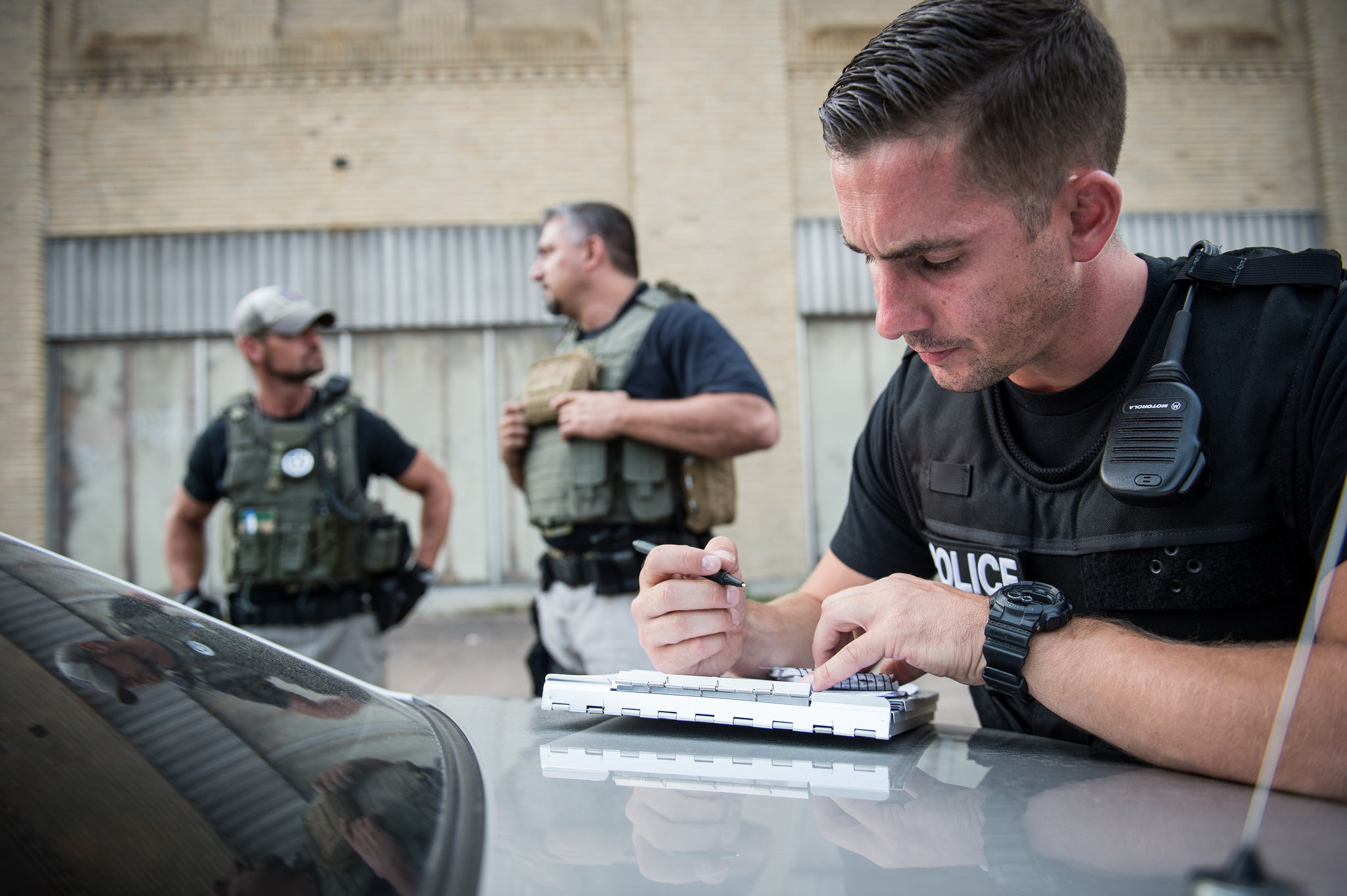
U.S. Marshals and police undertake Operation “Salt City” in Syracuse, New York, 2015. The actions led to 248 arrests and the seizure of cash, firearms, and drugs including heroin. Shane T. McCoy/US Marshals
Policing Families
Addiction becomes the pretext for a system of punitive social control over people whose long-standing poverty has made them objects of particular scorn. And it’s not just the medical and criminal justice systems. The Department of Children and Families is equally involved in many people’s lives. The head of DCF attributed the recent 40% increase in cases of children removed from their homes and placed in state custody to opiate addiction, despite data that indicates no statistically significant increase in opiate use in the state over the past decade. Children are being removed from their parents at such high rates that the Defender General had to hire several new attorneys just to handle these cases. Defense attorneys talked about the new “zero-tolerance” policies toward opiate-using mothers, how child protection staff and judges believe the opiate users they encounter are unfit parents solely because of their drug use. Once children are removed, parents face considerable obstacles in regaining custody. The combined conditions of stable housing, full-time employment, clean urinalysis, and regular attendance at drug counseling sessions (sometimes several a week), often without a car, prove insurmountable for many.
Through my years of research, I have observed a social control system of poor White drug users that resembles many of the findings in studies of poor addicts of color in urban areas. The experiences of poor White drug users in rural Vermont reveal the same “hostile exercise in disciplining” that anthropologist Phillipe Bourgois observed in his research among low-income African-American and Latino methadone patients in New York City and San Francisco. Their addictions were “disciplined” through a quasi-punitive and medical treatment model in much the same way the addictions of many White drug users in Vermont are.
Many of the people I’ve spoken with have had long-standing involvement with the criminal justice system. The enhanced cooperation among treatment and criminal justice has been strengthened because of the attention the opiate panic has received. This increased attention, in contrast to reports from suburban White America, has been accompanied by heightened policing. In June 2017, the Vera Institute of Justice released a report titled Out of Sight: The Growth of Jails in Rural America. It showed that the use of jails in rural areas has dramatically increased as it has declined in urban areas and asserted that this “new rurality of jails” is led, in part, by the growing incarceration of White people. Between 2004 and 2014, the percentage of White people in jail grew 19% in rural counties and 15% in small- and medium-sized cities. The New York Times has identified Dearborn County, Indiana as one of the most punitive places in the U.S. Over 97% of its inhabitants are White.
While violent crimes drive state and federal prison admissions, drug arrests and property crimes largely fuel the increase in admission to local rural jails. The criminal justice system does not collect information about social class, greatly limiting our ability to quantify the extent to which poverty plays a role in policing, prosecution, and sentencing decisions. But, from my research in Vermont and conversations with actors involved in the criminal justice system, I have seen how the mechanisms of social control deployed against poor White opiate users rely heavily on criminalization and look nothing like the “gentle” narrative portrayed in national media.
Jeff Sessions, currently the nation’s Attorney General, has made his intention clear: he will “aggressively prosecute” drug crimes. He has used the opiate crisis in his justification for no-tolerance policies. Local drug enforcement is not directly affected by federal policies but, given the rising rates of incarceration in rural America, there is little reason to doubt that county law enforcement will continue to jail its inhabitants, many of them White, at increasing rates. Political scientist Marie Gottschalk, in Caught, has argued that prisons are “resilient institutions” able to absorb critiques and emerge stronger. She points to arguments about racial bias, showing how some states simply increased their custodial control of White people to “equalize” incarceration rates between Whites and African Americans.
There are reasons to expect that White opiate users would receive better treatment than Black drug users, and much of the media rhetoric bolsters this assumption. But rhetoric is not reality in rural America. From New England to Appalachia, officials’ approaches to fighting opiates have largely involved a criminal justice response. Nor is the heightened punitive control of poor rural Whites new: The “meth panic” of the 1990s was accompanied by the criminalization of drug users, many White, in places like the Midwest. Again, the assumption that all White drug users are receiving better treatment because they are White ignores the stark class difference between suburban and rural drug users and the decades-long criminalized control of the latter. Poor White drug users complicate the dichotomies that characterize contemporary drug abuse discourse: poor and minority versus middle-class and White, prison versus treatment, addiction versus depravity.
It would appear that the long-standing poverty of many drug users in Vermont is itself being criminalized. As the superintendent of a local jail told me, most of the inmates are poor and they often need to come to jail to get stable housing and regular meals. “It’s sad,” he said, shaking his head, “it shouldn’t be this way.”
The national hand-wringing over opiates highlights the middle-class at a time when poor rural Whites are one of the fastest growing populations under criminal justice supervision. The media-framed drug panic obscures this inequality and exacerbates racial tension about the War on Drugs by focusing on the addictive drug that unites White opiate users rather than the class differences and inequality that divide them. As the criminal justice system modifies to withstand criticism, so too must those of us who care about drug policy and the effects of criminalization. Panic should not inform policy or displace the fact that criminalization reinforces class and race distinctions to the detriment of entire communities.
Recommended Readings
Caroline Acker. 2001. Creating the American Junkie: Addiction Research in the Classic Era of Narcotic Control. Baltimore, MD: Johns Hopkins University Press. A highly readable history of the first major U.S. opiate scare and the way in which medicine, psychiatry, and law combined to create the “junkie” figure so prominent in our cultural imagination.
Jason Cherkis. 2015. “Dying To Be Free,” Huffington Post, January 28. A multimedia essay illustrating the moral discourse that prevents heroin users from getting humane and life-saving treatment.
Marie Gottschalk. 2015. Caught: The Prison State and the Lockdown of American Politics. Oxford, UK: Oxford University Press. Gottschalk presents meticulously analyzed data about punishment trends, including those that affect poor rural Whites, to argue that reforms based on racial inequality or race neutrality will fail to address the prison state’s expansion.
Helena Hansen and Jules Netherland. 2017. “White Opioids: Pharmaceutical Race and the War on Drugs that Wasn’t,” Biosocieities 12(2). The authors argue that because the opiate panic is a “White drug war”, it’s characterized by a less punitive, more clinical approach than is customary of drug panics focused on people of color.
Craig Reinarman. 1994. “The Social Construction of Drug Scares,” in Peter Adler and Patricia Adler (eds), Constructions of Deviance. Belmont, CA: Wadsworth Publishing. A modern classic, this analysis of drug scares outlines their seven main ingredients and demonstrates that drug panics obscure the underlying racial and class tensions that precede them.
As America’s opiate epidemic rages on, calls for “treatment not punishment” dominate the national media. The hypocrisy of this response is not lost on a range of commentators: the reported move away from criminalization, they argue, is yet another example of racist drug policy. White people get treatment and poor people of color get punishment. Again.A cursory reading of national media seems to confirm this long-standing narrative of White, middle-class drug users as victims, not criminals. For example, the <em>New York Times’</em> coverage of suburban drug users has invited sympathy and identification with the people in the stories, encouraging the reader to see themselves, their child, or someone they know in the stories of good people raised in loving families who became opiate addicts almost by accident. The accompanying pictures to these articles show white people hugging as they leave drug treatment and well-dressed parents looking at pictures of the son or daughter they’ve lost to heroin. Photos of attractive and smiling teenagers—someone’s children—remind us of the promise and potential extinguished by an overdose. And yet, the <em>Times</em> is also savvy enough to contextualize this new drug panic when they write, “In Heroin Crisis, White Families Seek Gentler War on Drugs” (Oct. 30, 2015). They subtly remind the reader that non-White addicts get punishment and harshness when they refer to the White opiate crisis as a “new era” characterized by “striking shifts… some local police departments have stopped punishing many heroin users.” It is only because the users are White that a redemptive narrative of families and police coming together to stop opiate use can gain traction in print and in legislative bodies.And yet, this same media inadvertently invites a disruption to the dominant reading. In regional coverage of the opiate panic in Vermont, for example, the “crisis” of opiate use is framed as a “scourge” in quaint Bennington and in Rutland, a “blue-collar” town filled with addicts and drug dealers. The images accompanying these stories show a different tale of White drug use. Stephanie Predel, with dark circles under her eyes, is smoking a cigarette (itself a symbol of disrepute) in front of a ramshackle and dirty house. Alfred Hickey, looking tired and disheveled, is captioned to cast doubt: “[he] said he quit heroin.” Twenty-year-old Hailey Clark, here depicted as someone’s mother rather than daughter, is crying after losing custody of her son because of a heroin conviction. And two state troopers are pictured searching a suspect’s car for drugs. The story of opiates in Vermont is the opposite of innocence and community cohesion. As in suburban America, opiates are the culprit, but the response is markedly different. Poor White drug users get punishment.While media coverage hints at this differential treatment among White users, an almost exclusive focus on racial inequality in drug policy has been repeated without question by both drug policy reformers and scholars. For good reason, many are ready to see yet another example of racism in current drug policy: drug scares have a deeply racist history. The “crack epidemic” of the 1980s is a stark example of the way the fear of drugs was used to justify increased criminalized repression of people of color. The egregious sentencing disparity between crack (coded as a Black drug) and powder cocaine (coded as a White drug), emerged through bi-partisan Congressional consensus. Sentencing disparities by race remain a hallmark of the War on Drugs. The first drug scares in the U.S., which were also about opiates, were reflections of thinly veiled anti-Chinese racism in the late 19th and early 20th centuries. Drug prohibition often relies on the image of a demonized racial other whose drug use threatens social stability.But if we see only <em>racial</em> animus in drug scares, we overlook another engine of social control and harm: classism. The primary framing of the opiate epidemic as “White and middle-class” and the assumption that all White drug users have privilege serves to obscure the ways in which class figures prominently as a dividing line between which drug users are subjected to and exempted from punitive social control.For the past several years, I have studied the opiate panic in Vermont. I’ve lived in the town often referred to as “the heroin capital of New England”, talking with drug users, addiction medicine doctors, prosecutors, judges, defense attorneys, police and probation officers, jail superintendents, harm reduction providers, and community members, many of them neighbors. The notion that this is a “gentler drug war” conflicts with the punitive response I see in practice, in which poor White drug users are caught at the intersection of the criminal justice, drug treatment, and child protection systems.<dl id=”attachment_7514″ class=”wp-caption aligncenter” style=”width: 680px;” data-mce-style=”width: 680px;”><dt class=”wp-caption-dt”><a href=”https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k.jpg” data-mce-href=”https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k.jpg”><img class=”size-large wp-image-7514″ src=”https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k-680×453.jpg” alt=”” width=”680″ height=”453″ data-mce-src=”https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k-680×453.jpg” /></a></dt><dd class=”wp-caption-dd”>Pennsylvania’s governor, Tom Wolf, announces an expansion of a program to equip DCNR rangers with naloxone to reverse opioid overdoses. <a href=”https://flic.kr/p/SyBiiP” data-mce-href=”https://flic.kr/p/SyBiiP”>Governor Tom Wolf, Flickr CC</a></dd></dl>Pervasive CriminalizationSomething as simple as taking the bus to work, an hour and a half commute, turns into a lesson about life at the margins in a state governed by an opiate panic. Conversation inevitably turns to <em>why</em> someone is riding public transportation in a rural area where a vehicle is a necessity. I hear stories of people whose cars have been seized by the police, through asset forfeiture, returned to them so damaged from drug searches that the cars are beyond repair. People travel two hours south or north to meet with probation officers; an appointment in the afternoon means they might have to take the day off from work, spending several hours loitering in a local park or library until they can check in for the weekly supervision that costs them $100 a month. Lapses in regular ridership are often explained by a return to jail because of missed appointments with probation officers or positive drug tests.Poor White people are caught up in the system of punitive and medical control that relies heavily on the criminal justice system and its extension, compulsory drug treatment. People who came into the syringe exchange where I volunteered would complain that there were police officers waiting at the door to the methadone clinic around the corner. When I asked a clinic administrator about the cops, she reminded me that you can’t trust “these people… remember why they’re here.” And though she acknowledged that the clinic was providing a social service to sick people, it didn’t change the fact that many of their patients were also criminals. Law enforcement and social workers decide together how to respond to a “dirty urine” report from drug treatment (weekend stints in jail are a common consequence). On a recent trip to a county correctional facility, the superintendent told me that about 80% of the inmates were there for drug or drug-related charges. We pass through a dark hallway: as my eyes adjust, I see a figure in a cot in a small, unlit cell. This is the “medically managed detox”: I see three guards watching the man, but I am told a doctor is in the facility. For many rural drug users, the first “medical care” they receive is in jail.<dl id=”attachment_7515″ class=”wp-caption aligncenter” style=”width: 680px;” data-mce-style=”width: 680px;”><dt class=”wp-caption-dt”><a href=”https://contexts.org/files/2017/12/8095751137_4c16884965_b.jpg” data-mce-href=”https://contexts.org/files/2017/12/8095751137_4c16884965_b.jpg”><img class=”size-large wp-image-7515″ src=”https://contexts.org/files/2017/12/8095751137_4c16884965_b-680×636.jpg” alt=”” width=”680″ height=”636″ data-mce-src=”https://contexts.org/files/2017/12/8095751137_4c16884965_b-680×636.jpg” /></a></dt><dd class=”wp-caption-dd”>Many addicts began with legitimate prescriptions for pain medications, like Dilaudid, and turned to street drugs when their prescriptions were cut off. <a href=”https://flic.kr/p/dkoQLa” data-mce-href=”https://flic.kr/p/dkoQLa”>The.Comedian, Flickr CC</a></dd></dl>Punitive MedicalizationMuch of the media focus on the opiate panic in Vermont has centered on the willingness of the former governor, Peter Shumlin, to tackle the panic head-on by referring to it in his 2015 State of the State address. And Vermont is praised for its efforts to get drug users, especially those with criminal convictions, into “medically assisted treatment” (opiate replacement therapy such as methadone or buprenorphine) quickly. The reality for the drug users I’ve spoken with is that this approach, praised by many treatment providers and advocates across the country as an “enlightened” way to treat opiate addiction, becomes another form of control.“Heroin or nothing,” as Steven, a man I met at the syringe exchange, put it. Those were his options. He’d broken his back several years before, and opiates helped with the lasting pain as he continued in manual labor, working odd jobs and moving furniture. But treating the physical pain now meant dealing with the “pain in the ass” of the system, of the methadone treatment providers and probation officers. Steven was among the many people I encountered who had initially started using legally obtained opiates to treat pain from work-related injuries, only to find their access limited by increasingly stringent state prescribing regulations. People like Steven turned to heroin not because they preferred it, but because they could no longer get prescription painkillers.Conversations with addiction medicine providers echo the judgment about which some of the drug users I’ve spoken with complain. In the <em>New York Times’</em> coverage of the suburban opiate panic, doctors identify with their patients, perhaps even knowing them socially. This is not the case in Vermont, where the class divide between doctors and patients is wide. Even the most sympathetic physicians I spoke with endorsed monitoring and coerced treatment. One said that there was “no high-level thinking in Vermont” and “no one understands the medical piece.” When I asked about the best way to treat addiction, this doctor told me it was suboxone (buprenorphine) combined with “tight control… put an ankle bracelet on them and tightly monitor them… If you mess up, you go to jail. Folks do best when there are consequences.” Other medical providers were frustrated with their patients, viewing their poverty-related struggles such as lack of transportation or difficulty finding employment as “excuses” for not succeeding in recovery. Their patients’ continued smoking and poor eating habits are also a regular source of frustration. One doctor who called addiction a “disease” insists that the criminal justice oversight of a sick person is not a contradiction, but a mechanism to ensure sorely needed “accountability.”In my book <em>Judging Addicts</em>, I detailed the merger of the medical and punitive frameworks of addiction and how they’ve come to characterize the modern treatment system in the U.S.: criminalization and medicalization are complementary, rather than contradictory approaches, I argued. This merger is apparent in Vermont where the treatment and punishment systems are deeply intertwined. And yet, this mingling has not necessarily led law enforcement to a more progressive or lenient view of addicts or for medical providers to argue that addicts shouldn’t be criminally punished. A prosecutor who was assigned to a drug court told me: “Their problem isn’t really addiction, their problem is that they’re criminals. And their parents were criminals.” This person was reluctant to accept the narrative that these people were sick even though she was working as part of a Drug Court Team whose ostensible goal was to get addicts the services they need to become drug and alcohol, and thus crime, free.<dl id=”attachment_7516″ class=”wp-caption aligncenter” style=”width: 680px;” data-mce-style=”width: 680px;”><dt class=”wp-caption-dt”><a href=”https://contexts.org/files/2017/12/20626846824_18ad3414a4_k.jpg” data-mce-href=”https://contexts.org/files/2017/12/20626846824_18ad3414a4_k.jpg”><img class=”size-large wp-image-7516″ src=”https://contexts.org/files/2017/12/20626846824_18ad3414a4_k-680×453.jpg” alt=”” width=”680″ height=”453″ data-mce-src=”https://contexts.org/files/2017/12/20626846824_18ad3414a4_k-680×453.jpg” /></a></dt><dd class=”wp-caption-dd”>U.S. Marshals and police undertake Operation “Salt City” in Syracuse, New York, 2015. The actions led to 248 arrests and the seizure of cash, firearms, and drugs including heroin. <a href=”https://flic.kr/p/xqHYW5″ data-mce-href=”https://flic.kr/p/xqHYW5″>Shane T. McCoy/US Marshals</a></dd></dl>Policing FamiliesAddiction becomes the pretext for a system of punitive social control over people whose long-standing poverty has made them objects of particular scorn. And it’s not just the medical and criminal justice systems. The Department of Children and Families is equally involved in many people’s lives. The head of DCF attributed the recent 40% increase in cases of children removed from their homes and placed in state custody to opiate addiction, despite data that indicates no statistically significant increase in opiate use in the state over the past decade. Children are being removed from their parents at such high rates that the Defender General had to hire several new attorneys just to handle these cases. Defense attorneys talked about the new “zero-tolerance” policies toward opiate-using mothers, how child protection staff and judges believe the opiate users they encounter are unfit parents solely because of their drug use. Once children are removed, parents face considerable obstacles in regaining custody. The combined conditions of stable housing, full-time employment, clean urinalysis, and regular attendance at drug counseling sessions (sometimes several a week), often without a car, prove insurmountable for many.Through my years of research, I have observed a social control system of poor White drug users that resembles many of the findings in studies of poor addicts of color in urban areas. The experiences of poor White drug users in rural Vermont reveal the same “hostile exercise in disciplining” that anthropologist Phillipe Bourgois observed in his research among low-income African-American and Latino methadone patients in New York City and San Francisco. Their addictions were “disciplined” through a quasi-punitive and medical treatment model in much the same way the addictions of many White drug users in Vermont are.<dl id=”attachment_7517″ class=”wp-caption aligncenter” style=”width: 300px;” data-mce-style=”width: 300px;”><dt class=”wp-caption-dt”><a href=”https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388.jpg” data-mce-href=”https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388.jpg”><img class=”size-medium wp-image-7517″ src=”https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388-300×270.jpg” alt=”” width=”300″ height=”270″ data-mce-src=”https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388-300×270.jpg” /></a></dt><dd class=”wp-caption-dd”>A woman holds up a photo of her son at a “Heroin Summit” with the Lt. Governor of Maryland. <a href=”https://flic.kr/p/sVMCH2″ data-mce-href=”https://flic.kr/p/sVMCH2″>Joe Andrucyk, MarylandGovPics, Flickr CC</a></dd></dl>Expanding PunishmentMany of the people I’ve spoken with have had long-standing involvement with the criminal justice system. The enhanced cooperation among treatment and criminal justice has been strengthened because of the attention the opiate panic has received. This increased attention, in contrast to reports from suburban White America, has been accompanied by heightened policing. In June 2017, the Vera Institute of Justice released a report titled <em>Out of Sight: The Growth of Jails in Rural America</em>. It showed that the use of jails in rural areas has dramatically increased as it has declined in urban areas and asserted that this “new rurality of jails” is led, in part, by the growing incarceration of White people. Between 2004 and 2014, the percentage of White people in jail grew 19% in rural counties and 15% in small- and medium-sized cities. The <em>New York Times</em> has identified Dearborn County, Indiana as one of the most punitive places in the U.S. Over 97% of its inhabitants are White.While violent crimes drive state and federal prison admissions, drug arrests and property crimes largely fuel the increase in admission to local rural jails. The criminal justice system does not collect information about social class, greatly limiting our ability to quantify the extent to which poverty plays a role in policing, prosecution, and sentencing decisions. But, from my research in Vermont and conversations with actors involved in the criminal justice system, I have seen how the mechanisms of social control deployed against poor White opiate users rely heavily on criminalization and look nothing like the “gentle” narrative portrayed in national media.Jeff Sessions, currently the nation’s Attorney General, has made his intention clear: he will “aggressively prosecute” drug crimes. He has used the opiate crisis in his justification for no-tolerance policies. Local drug enforcement is not directly affected by federal policies but, given the rising rates of incarceration in rural America, there is little reason to doubt that county law enforcement will continue to jail its inhabitants, many of them White, at increasing rates. Political scientist Marie Gottschalk, in <em>Caught</em>, has argued that prisons are “resilient institutions” able to absorb critiques and emerge stronger. She points to arguments about racial bias, showing how some states simply increased their custodial control of White people to “equalize” incarceration rates between Whites and African Americans.There are reasons to expect that White opiate users would receive better treatment than Black drug users, and much of the media rhetoric bolsters this assumption. But rhetoric is not reality in rural America. From New England to Appalachia, officials’ approaches to fighting opiates have largely involved a criminal justice response. Nor is the heightened punitive control of poor rural Whites new: The “meth panic” of the 1990s was accompanied by the criminalization of drug users, many White, in places like the Midwest. Again, the assumption that all White drug users are receiving better treatment because they are White ignores the stark class difference between suburban and rural drug users and the decades-long criminalized control of the latter. Poor White drug users complicate the dichotomies that characterize contemporary drug abuse discourse: poor and minority versus middle-class and White, prison versus treatment, addiction versus depravity.It would appear that the long-standing poverty of many drug users in Vermont is itself being criminalized. As the superintendent of a local jail told me, most of the inmates are poor and they often need to come to jail to get stable housing and regular meals. “It’s sad,” he said, shaking his head, “it shouldn’t be this way.”The national hand-wringing over opiates highlights the middle-class at a time when poor rural Whites are one of the fastest growing populations under criminal justice supervision. The media-framed drug panic obscures this inequality and exacerbates racial tension about the War on Drugs by focusing on the addictive drug that unites White opiate users rather than the class differences and inequality that divide them. As the criminal justice system modifies to withstand criticism, so too must those of us who care about drug policy and the effects of criminalization. Panic should not inform policy or displace the fact that criminalization reinforces class and race distinctions to the detriment of entire communities.Recommended ReadingsCaroline Acker. 2001. <em>Creating the American Junkie: Addiction Research in the Classic Era of Narcotic Control.</em> Baltimore, MD: Johns Hopkins University Press. A highly readable history of the first major U.S. opiate scare and the way in which medicine, psychiatry, and law combined to create the “junkie” figure so prominent in our cultural imagination.Jason Cherkis. 2015. “Dying To Be Free,” <em>Huffington Post</em>, January 28. A multimedia essay illustrating the moral discourse that prevents heroin users from getting humane and life-saving treatment.Marie Gottschalk. 2015. <em>Caught: The Prison State and the Lockdown of American Politics.</em> Oxford, UK: Oxford University Press. Gottschalk presents meticulously analyzed data about punishment trends, including those that affect poor rural Whites, to argue that reforms based on racial inequality or race neutrality will fail to address the prison state’s expansion.Helena Hansen and Jules Netherland. 2017. “White Opioids: Pharmaceutical Race and the War on Drugs that Wasn’t,” <em>Biosocieities</em> 12(2). The authors argue that because the opiate panic is a “White drug war”, it’s characterized by a less punitive, more clinical approach than is customary of drug panics focused on people of color.Craig Reinarman. 1994. “The Social Construction of Drug Scares,” in Peter Adler and Patricia Adler (eds), <em>Constructions of Deviance</em>. Belmont, CA: Wadsworth Publishing. A modern classic, this analysis of drug scares outlines their seven main ingredients and demonstrates that drug panics obscure the underlying racial and class tensions that precede them.
Author
As America’s opiate epidemic rages on, calls for “treatment not punishment” dominate the national media. The hypocrisy of this response is not lost on a range of commentators: the reported move away from criminalization, they argue, is yet another example of racist drug policy. White people get treatment and poor people of color get punishment. Again.A cursory reading of national media seems to confirm this long-standing narrative of White, middle-class drug users as victims, not criminals. For example, the <em>New York Times’</em> coverage of suburban drug users has invited sympathy and identification with the people in the stories, encouraging the reader to see themselves, their child, or someone they know in the stories of good people raised in loving families who became opiate addicts almost by accident. The accompanying pictures to these articles show white people hugging as they leave drug treatment and well-dressed parents looking at pictures of the son or daughter they’ve lost to heroin. Photos of attractive and smiling teenagers—someone’s children—remind us of the promise and potential extinguished by an overdose. And yet, the <em>Times</em> is also savvy enough to contextualize this new drug panic when they write, “In Heroin Crisis, White Families Seek Gentler War on Drugs” (Oct. 30, 2015). They subtly remind the reader that non-White addicts get punishment and harshness when they refer to the White opiate crisis as a “new era” characterized by “striking shifts… some local police departments have stopped punishing many heroin users.” It is only because the users are White that a redemptive narrative of families and police coming together to stop opiate use can gain traction in print and in legislative bodies.And yet, this same media inadvertently invites a disruption to the dominant reading. In regional coverage of the opiate panic in Vermont, for example, the “crisis” of opiate use is framed as a “scourge” in quaint Bennington and in Rutland, a “blue-collar” town filled with addicts and drug dealers. The images accompanying these stories show a different tale of White drug use. Stephanie Predel, with dark circles under her eyes, is smoking a cigarette (itself a symbol of disrepute) in front of a ramshackle and dirty house. Alfred Hickey, looking tired and disheveled, is captioned to cast doubt: “[he] said he quit heroin.” Twenty-year-old Hailey Clark, here depicted as someone’s mother rather than daughter, is crying after losing custody of her son because of a heroin conviction. And two state troopers are pictured searching a suspect’s car for drugs. The story of opiates in Vermont is the opposite of innocence and community cohesion. As in suburban America, opiates are the culprit, but the response is markedly different. Poor White drug users get punishment.While media coverage hints at this differential treatment among White users, an almost exclusive focus on racial inequality in drug policy has been repeated without question by both drug policy reformers and scholars. For good reason, many are ready to see yet another example of racism in current drug policy: drug scares have a deeply racist history. The “crack epidemic” of the 1980s is a stark example of the way the fear of drugs was used to justify increased criminalized repression of people of color. The egregious sentencing disparity between crack (coded as a Black drug) and powder cocaine (coded as a White drug), emerged through bi-partisan Congressional consensus. Sentencing disparities by race remain a hallmark of the War on Drugs. The first drug scares in the U.S., which were also about opiates, were reflections of thinly veiled anti-Chinese racism in the late 19th and early 20th centuries. Drug prohibition often relies on the image of a demonized racial other whose drug use threatens social stability.But if we see only <em>racial</em> animus in drug scares, we overlook another engine of social control and harm: classism. The primary framing of the opiate epidemic as “White and middle-class” and the assumption that all White drug users have privilege serves to obscure the ways in which class figures prominently as a dividing line between which drug users are subjected to and exempted from punitive social control.For the past several years, I have studied the opiate panic in Vermont. I’ve lived in the town often referred to as “the heroin capital of New England”, talking with drug users, addiction medicine doctors, prosecutors, judges, defense attorneys, police and probation officers, jail superintendents, harm reduction providers, and community members, many of them neighbors. The notion that this is a “gentler drug war” conflicts with the punitive response I see in practice, in which poor White drug users are caught at the intersection of the criminal justice, drug treatment, and child protection systems.<dl id="attachment_7514" class="wp-caption aligncenter" style="width: 680px;" data-mce-style="width: 680px;"><dt class="wp-caption-dt"><a href="https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k.jpg" data-mce-href="https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k.jpg"><img class="size-large wp-image-7514" src="https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k-680x453.jpg" alt="" width="680" height="453" data-mce-src="https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k-680x453.jpg" /></a></dt><dd class="wp-caption-dd">Pennsylvania's governor, Tom Wolf, announces an expansion of a program to equip DCNR rangers with naloxone to reverse opioid overdoses. <a href="https://flic.kr/p/SyBiiP" data-mce-href="https://flic.kr/p/SyBiiP">Governor Tom Wolf, Flickr CC</a></dd></dl>Pervasive CriminalizationSomething as simple as taking the bus to work, an hour and a half commute, turns into a lesson about life at the margins in a state governed by an opiate panic. Conversation inevitably turns to <em>why</em> someone is riding public transportation in a rural area where a vehicle is a necessity. I hear stories of people whose cars have been seized by the police, through asset forfeiture, returned to them so damaged from drug searches that the cars are beyond repair. People travel two hours south or north to meet with probation officers; an appointment in the afternoon means they might have to take the day off from work, spending several hours loitering in a local park or library until they can check in for the weekly supervision that costs them $100 a month. Lapses in regular ridership are often explained by a return to jail because of missed appointments with probation officers or positive drug tests.Poor White people are caught up in the system of punitive and medical control that relies heavily on the criminal justice system and its extension, compulsory drug treatment. People who came into the syringe exchange where I volunteered would complain that there were police officers waiting at the door to the methadone clinic around the corner. When I asked a clinic administrator about the cops, she reminded me that you can’t trust “these people… remember why they’re here.” And though she acknowledged that the clinic was providing a social service to sick people, it didn’t change the fact that many of their patients were also criminals. Law enforcement and social workers decide together how to respond to a “dirty urine” report from drug treatment (weekend stints in jail are a common consequence). On a recent trip to a county correctional facility, the superintendent told me that about 80% of the inmates were there for drug or drug-related charges. We pass through a dark hallway: as my eyes adjust, I see a figure in a cot in a small, unlit cell. This is the “medically managed detox”: I see three guards watching the man, but I am told a doctor is in the facility. For many rural drug users, the first “medical care” they receive is in jail.<dl id="attachment_7515" class="wp-caption aligncenter" style="width: 680px;" data-mce-style="width: 680px;"><dt class="wp-caption-dt"><a href="https://contexts.org/files/2017/12/8095751137_4c16884965_b.jpg" data-mce-href="https://contexts.org/files/2017/12/8095751137_4c16884965_b.jpg"><img class="size-large wp-image-7515" src="https://contexts.org/files/2017/12/8095751137_4c16884965_b-680x636.jpg" alt="" width="680" height="636" data-mce-src="https://contexts.org/files/2017/12/8095751137_4c16884965_b-680x636.jpg" /></a></dt><dd class="wp-caption-dd">Many addicts began with legitimate prescriptions for pain medications, like Dilaudid, and turned to street drugs when their prescriptions were cut off. <a href="https://flic.kr/p/dkoQLa" data-mce-href="https://flic.kr/p/dkoQLa">The.Comedian, Flickr CC</a></dd></dl>Punitive MedicalizationMuch of the media focus on the opiate panic in Vermont has centered on the willingness of the former governor, Peter Shumlin, to tackle the panic head-on by referring to it in his 2015 State of the State address. And Vermont is praised for its efforts to get drug users, especially those with criminal convictions, into “medically assisted treatment” (opiate replacement therapy such as methadone or buprenorphine) quickly. The reality for the drug users I’ve spoken with is that this approach, praised by many treatment providers and advocates across the country as an “enlightened” way to treat opiate addiction, becomes another form of control.“Heroin or nothing,” as Steven, a man I met at the syringe exchange, put it. Those were his options. He’d broken his back several years before, and opiates helped with the lasting pain as he continued in manual labor, working odd jobs and moving furniture. But treating the physical pain now meant dealing with the “pain in the ass” of the system, of the methadone treatment providers and probation officers. Steven was among the many people I encountered who had initially started using legally obtained opiates to treat pain from work-related injuries, only to find their access limited by increasingly stringent state prescribing regulations. People like Steven turned to heroin not because they preferred it, but because they could no longer get prescription painkillers.Conversations with addiction medicine providers echo the judgment about which some of the drug users I’ve spoken with complain. In the <em>New York Times’</em> coverage of the suburban opiate panic, doctors identify with their patients, perhaps even knowing them socially. This is not the case in Vermont, where the class divide between doctors and patients is wide. Even the most sympathetic physicians I spoke with endorsed monitoring and coerced treatment. One said that there was “no high-level thinking in Vermont” and “no one understands the medical piece.” When I asked about the best way to treat addiction, this doctor told me it was suboxone (buprenorphine) combined with “tight control… put an ankle bracelet on them and tightly monitor them… If you mess up, you go to jail. Folks do best when there are consequences.” Other medical providers were frustrated with their patients, viewing their poverty-related struggles such as lack of transportation or difficulty finding employment as “excuses” for not succeeding in recovery. Their patients’ continued smoking and poor eating habits are also a regular source of frustration. One doctor who called addiction a “disease” insists that the criminal justice oversight of a sick person is not a contradiction, but a mechanism to ensure sorely needed “accountability.”In my book <em>Judging Addicts</em>, I detailed the merger of the medical and punitive frameworks of addiction and how they’ve come to characterize the modern treatment system in the U.S.: criminalization and medicalization are complementary, rather than contradictory approaches, I argued. This merger is apparent in Vermont where the treatment and punishment systems are deeply intertwined. And yet, this mingling has not necessarily led law enforcement to a more progressive or lenient view of addicts or for medical providers to argue that addicts shouldn’t be criminally punished. A prosecutor who was assigned to a drug court told me: “Their problem isn’t really addiction, their problem is that they’re criminals. And their parents were criminals.” This person was reluctant to accept the narrative that these people were sick even though she was working as part of a Drug Court Team whose ostensible goal was to get addicts the services they need to become drug and alcohol, and thus crime, free.<dl id="attachment_7516" class="wp-caption aligncenter" style="width: 680px;" data-mce-style="width: 680px;"><dt class="wp-caption-dt"><a href="https://contexts.org/files/2017/12/20626846824_18ad3414a4_k.jpg" data-mce-href="https://contexts.org/files/2017/12/20626846824_18ad3414a4_k.jpg"><img class="size-large wp-image-7516" src="https://contexts.org/files/2017/12/20626846824_18ad3414a4_k-680x453.jpg" alt="" width="680" height="453" data-mce-src="https://contexts.org/files/2017/12/20626846824_18ad3414a4_k-680x453.jpg" /></a></dt><dd class="wp-caption-dd">U.S. Marshals and police undertake Operation "Salt City" in Syracuse, New York, 2015. The actions led to 248 arrests and the seizure of cash, firearms, and drugs including heroin. <a href="https://flic.kr/p/xqHYW5" data-mce-href="https://flic.kr/p/xqHYW5">Shane T. McCoy/US Marshals</a></dd></dl>Policing FamiliesAddiction becomes the pretext for a system of punitive social control over people whose long-standing poverty has made them objects of particular scorn. And it’s not just the medical and criminal justice systems. The Department of Children and Families is equally involved in many people’s lives. The head of DCF attributed the recent 40% increase in cases of children removed from their homes and placed in state custody to opiate addiction, despite data that indicates no statistically significant increase in opiate use in the state over the past decade. Children are being removed from their parents at such high rates that the Defender General had to hire several new attorneys just to handle these cases. Defense attorneys talked about the new “zero-tolerance” policies toward opiate-using mothers, how child protection staff and judges believe the opiate users they encounter are unfit parents solely because of their drug use. Once children are removed, parents face considerable obstacles in regaining custody. The combined conditions of stable housing, full-time employment, clean urinalysis, and regular attendance at drug counseling sessions (sometimes several a week), often without a car, prove insurmountable for many.Through my years of research, I have observed a social control system of poor White drug users that resembles many of the findings in studies of poor addicts of color in urban areas. The experiences of poor White drug users in rural Vermont reveal the same “hostile exercise in disciplining” that anthropologist Phillipe Bourgois observed in his research among low-income African-American and Latino methadone patients in New York City and San Francisco. Their addictions were “disciplined” through a quasi-punitive and medical treatment model in much the same way the addictions of many White drug users in Vermont are.<dl id="attachment_7517" class="wp-caption aligncenter" style="width: 300px;" data-mce-style="width: 300px;"><dt class="wp-caption-dt"><a href="https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388.jpg" data-mce-href="https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388.jpg"><img class="size-medium wp-image-7517" src="https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388-300x270.jpg" alt="" width="300" height="270" data-mce-src="https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388-300x270.jpg" /></a></dt><dd class="wp-caption-dd">A woman holds up a photo of her son at a "Heroin Summit" with the Lt. Governor of Maryland. <a href="https://flic.kr/p/sVMCH2" data-mce-href="https://flic.kr/p/sVMCH2">Joe Andrucyk, MarylandGovPics, Flickr CC</a></dd></dl>Expanding PunishmentMany of the people I’ve spoken with have had long-standing involvement with the criminal justice system. The enhanced cooperation among treatment and criminal justice has been strengthened because of the attention the opiate panic has received. This increased attention, in contrast to reports from suburban White America, has been accompanied by heightened policing. In June 2017, the Vera Institute of Justice released a report titled <em>Out of Sight: The Growth of Jails in Rural America</em>. It showed that the use of jails in rural areas has dramatically increased as it has declined in urban areas and asserted that this “new rurality of jails” is led, in part, by the growing incarceration of White people. Between 2004 and 2014, the percentage of White people in jail grew 19% in rural counties and 15% in small- and medium-sized cities. The <em>New York Times</em> has identified Dearborn County, Indiana as one of the most punitive places in the U.S. Over 97% of its inhabitants are White.While violent crimes drive state and federal prison admissions, drug arrests and property crimes largely fuel the increase in admission to local rural jails. The criminal justice system does not collect information about social class, greatly limiting our ability to quantify the extent to which poverty plays a role in policing, prosecution, and sentencing decisions. But, from my research in Vermont and conversations with actors involved in the criminal justice system, I have seen how the mechanisms of social control deployed against poor White opiate users rely heavily on criminalization and look nothing like the “gentle” narrative portrayed in national media.Jeff Sessions, currently the nation’s Attorney General, has made his intention clear: he will “aggressively prosecute” drug crimes. He has used the opiate crisis in his justification for no-tolerance policies. Local drug enforcement is not directly affected by federal policies but, given the rising rates of incarceration in rural America, there is little reason to doubt that county law enforcement will continue to jail its inhabitants, many of them White, at increasing rates. Political scientist Marie Gottschalk, in <em>Caught</em>, has argued that prisons are “resilient institutions” able to absorb critiques and emerge stronger. She points to arguments about racial bias, showing how some states simply increased their custodial control of White people to “equalize” incarceration rates between Whites and African Americans.There are reasons to expect that White opiate users would receive better treatment than Black drug users, and much of the media rhetoric bolsters this assumption. But rhetoric is not reality in rural America. From New England to Appalachia, officials’ approaches to fighting opiates have largely involved a criminal justice response. Nor is the heightened punitive control of poor rural Whites new: The “meth panic” of the 1990s was accompanied by the criminalization of drug users, many White, in places like the Midwest. Again, the assumption that all White drug users are receiving better treatment because they are White ignores the stark class difference between suburban and rural drug users and the decades-long criminalized control of the latter. Poor White drug users complicate the dichotomies that characterize contemporary drug abuse discourse: poor and minority versus middle-class and White, prison versus treatment, addiction versus depravity.It would appear that the long-standing poverty of many drug users in Vermont is itself being criminalized. As the superintendent of a local jail told me, most of the inmates are poor and they often need to come to jail to get stable housing and regular meals. “It’s sad,” he said, shaking his head, “it shouldn’t be this way.”The national hand-wringing over opiates highlights the middle-class at a time when poor rural Whites are one of the fastest growing populations under criminal justice supervision. The media-framed drug panic obscures this inequality and exacerbates racial tension about the War on Drugs by focusing on the addictive drug that unites White opiate users rather than the class differences and inequality that divide them. As the criminal justice system modifies to withstand criticism, so too must those of us who care about drug policy and the effects of criminalization. Panic should not inform policy or displace the fact that criminalization reinforces class and race distinctions to the detriment of entire communities.Recommended ReadingsCaroline Acker. 2001. <em>Creating the American Junkie: Addiction Research in the Classic Era of Narcotic Control.</em> Baltimore, MD: Johns Hopkins University Press. A highly readable history of the first major U.S. opiate scare and the way in which medicine, psychiatry, and law combined to create the “junkie” figure so prominent in our cultural imagination.Jason Cherkis. 2015. “Dying To Be Free,” <em>Huffington Post</em>, January 28. A multimedia essay illustrating the moral discourse that prevents heroin users from getting humane and life-saving treatment.Marie Gottschalk. 2015. <em>Caught: The Prison State and the Lockdown of American Politics.</em> Oxford, UK: Oxford University Press. Gottschalk presents meticulously analyzed data about punishment trends, including those that affect poor rural Whites, to argue that reforms based on racial inequality or race neutrality will fail to address the prison state’s expansion.Helena Hansen and Jules Netherland. 2017. “White Opioids: Pharmaceutical Race and the War on Drugs that Wasn’t,” <em>Biosocieities</em> 12(2). The authors argue that because the opiate panic is a “White drug war”, it’s characterized by a less punitive, more clinical approach than is customary of drug panics focused on people of color.Craig Reinarman. 1994. “The Social Construction of Drug Scares,” in Peter Adler and Patricia Adler (eds), <em>Constructions of Deviance</em>. Belmont, CA: Wadsworth Publishing. A modern classic, this analysis of drug scares outlines their seven main ingredients and demonstrates that drug panics obscure the underlying racial and class tensions that precede them.
As America’s opiate epidemic rages on, calls for “treatment not punishment” dominate the national media. The hypocrisy of this response is not lost on a range of commentators: the reported move away from criminalization, they argue, is yet another example of racist drug policy. White people get treatment and poor people of color get punishment. Again.A cursory reading of national media seems to confirm this long-standing narrative of White, middle-class drug users as victims, not criminals. For example, the <em>New York Times’</em> coverage of suburban drug users has invited sympathy and identification with the people in the stories, encouraging the reader to see themselves, their child, or someone they know in the stories of good people raised in loving families who became opiate addicts almost by accident. The accompanying pictures to these articles show white people hugging as they leave drug treatment and well-dressed parents looking at pictures of the son or daughter they’ve lost to heroin. Photos of attractive and smiling teenagers—someone’s children—remind us of the promise and potential extinguished by an overdose. And yet, the <em>Times</em> is also savvy enough to contextualize this new drug panic when they write, “In Heroin Crisis, White Families Seek Gentler War on Drugs” (Oct. 30, 2015). They subtly remind the reader that non-White addicts get punishment and harshness when they refer to the White opiate crisis as a “new era” characterized by “striking shifts… some local police departments have stopped punishing many heroin users.” It is only because the users are White that a redemptive narrative of families and police coming together to stop opiate use can gain traction in print and in legislative bodies.And yet, this same media inadvertently invites a disruption to the dominant reading. In regional coverage of the opiate panic in Vermont, for example, the “crisis” of opiate use is framed as a “scourge” in quaint Bennington and in Rutland, a “blue-collar” town filled with addicts and drug dealers. The images accompanying these stories show a different tale of White drug use. Stephanie Predel, with dark circles under her eyes, is smoking a cigarette (itself a symbol of disrepute) in front of a ramshackle and dirty house. Alfred Hickey, looking tired and disheveled, is captioned to cast doubt: “[he] said he quit heroin.” Twenty-year-old Hailey Clark, here depicted as someone’s mother rather than daughter, is crying after losing custody of her son because of a heroin conviction. And two state troopers are pictured searching a suspect’s car for drugs. The story of opiates in Vermont is the opposite of innocence and community cohesion. As in suburban America, opiates are the culprit, but the response is markedly different. Poor White drug users get punishment.While media coverage hints at this differential treatment among White users, an almost exclusive focus on racial inequality in drug policy has been repeated without question by both drug policy reformers and scholars. For good reason, many are ready to see yet another example of racism in current drug policy: drug scares have a deeply racist history. The “crack epidemic” of the 1980s is a stark example of the way the fear of drugs was used to justify increased criminalized repression of people of color. The egregious sentencing disparity between crack (coded as a Black drug) and powder cocaine (coded as a White drug), emerged through bi-partisan Congressional consensus. Sentencing disparities by race remain a hallmark of the War on Drugs. The first drug scares in the U.S., which were also about opiates, were reflections of thinly veiled anti-Chinese racism in the late 19th and early 20th centuries. Drug prohibition often relies on the image of a demonized racial other whose drug use threatens social stability.But if we see only <em>racial</em> animus in drug scares, we overlook another engine of social control and harm: classism. The primary framing of the opiate epidemic as “White and middle-class” and the assumption that all White drug users have privilege serves to obscure the ways in which class figures prominently as a dividing line between which drug users are subjected to and exempted from punitive social control.For the past several years, I have studied the opiate panic in Vermont. I’ve lived in the town often referred to as “the heroin capital of New England”, talking with drug users, addiction medicine doctors, prosecutors, judges, defense attorneys, police and probation officers, jail superintendents, harm reduction providers, and community members, many of them neighbors. The notion that this is a “gentler drug war” conflicts with the punitive response I see in practice, in which poor White drug users are caught at the intersection of the criminal justice, drug treatment, and child protection systems.<dl id="attachment_7514" class="wp-caption aligncenter" style="width: 680px;" data-mce-style="width: 680px;"><dt class="wp-caption-dt"><a href="https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k.jpg" data-mce-href="https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k.jpg"><img class="size-large wp-image-7514" src="https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k-680x453.jpg" alt="" width="680" height="453" data-mce-src="https://contexts.org/files/2017/12/33186853413_ac46e71c1a_k-680x453.jpg" /></a></dt><dd class="wp-caption-dd">Pennsylvania's governor, Tom Wolf, announces an expansion of a program to equip DCNR rangers with naloxone to reverse opioid overdoses. <a href="https://flic.kr/p/SyBiiP" data-mce-href="https://flic.kr/p/SyBiiP">Governor Tom Wolf, Flickr CC</a></dd></dl>Pervasive CriminalizationSomething as simple as taking the bus to work, an hour and a half commute, turns into a lesson about life at the margins in a state governed by an opiate panic. Conversation inevitably turns to <em>why</em> someone is riding public transportation in a rural area where a vehicle is a necessity. I hear stories of people whose cars have been seized by the police, through asset forfeiture, returned to them so damaged from drug searches that the cars are beyond repair. People travel two hours south or north to meet with probation officers; an appointment in the afternoon means they might have to take the day off from work, spending several hours loitering in a local park or library until they can check in for the weekly supervision that costs them $100 a month. Lapses in regular ridership are often explained by a return to jail because of missed appointments with probation officers or positive drug tests.Poor White people are caught up in the system of punitive and medical control that relies heavily on the criminal justice system and its extension, compulsory drug treatment. People who came into the syringe exchange where I volunteered would complain that there were police officers waiting at the door to the methadone clinic around the corner. When I asked a clinic administrator about the cops, she reminded me that you can’t trust “these people… remember why they’re here.” And though she acknowledged that the clinic was providing a social service to sick people, it didn’t change the fact that many of their patients were also criminals. Law enforcement and social workers decide together how to respond to a “dirty urine” report from drug treatment (weekend stints in jail are a common consequence). On a recent trip to a county correctional facility, the superintendent told me that about 80% of the inmates were there for drug or drug-related charges. We pass through a dark hallway: as my eyes adjust, I see a figure in a cot in a small, unlit cell. This is the “medically managed detox”: I see three guards watching the man, but I am told a doctor is in the facility. For many rural drug users, the first “medical care” they receive is in jail.<dl id="attachment_7515" class="wp-caption aligncenter" style="width: 680px;" data-mce-style="width: 680px;"><dt class="wp-caption-dt"><a href="https://contexts.org/files/2017/12/8095751137_4c16884965_b.jpg" data-mce-href="https://contexts.org/files/2017/12/8095751137_4c16884965_b.jpg"><img class="size-large wp-image-7515" src="https://contexts.org/files/2017/12/8095751137_4c16884965_b-680x636.jpg" alt="" width="680" height="636" data-mce-src="https://contexts.org/files/2017/12/8095751137_4c16884965_b-680x636.jpg" /></a></dt><dd class="wp-caption-dd">Many addicts began with legitimate prescriptions for pain medications, like Dilaudid, and turned to street drugs when their prescriptions were cut off. <a href="https://flic.kr/p/dkoQLa" data-mce-href="https://flic.kr/p/dkoQLa">The.Comedian, Flickr CC</a></dd></dl>Punitive MedicalizationMuch of the media focus on the opiate panic in Vermont has centered on the willingness of the former governor, Peter Shumlin, to tackle the panic head-on by referring to it in his 2015 State of the State address. And Vermont is praised for its efforts to get drug users, especially those with criminal convictions, into “medically assisted treatment” (opiate replacement therapy such as methadone or buprenorphine) quickly. The reality for the drug users I’ve spoken with is that this approach, praised by many treatment providers and advocates across the country as an “enlightened” way to treat opiate addiction, becomes another form of control.“Heroin or nothing,” as Steven, a man I met at the syringe exchange, put it. Those were his options. He’d broken his back several years before, and opiates helped with the lasting pain as he continued in manual labor, working odd jobs and moving furniture. But treating the physical pain now meant dealing with the “pain in the ass” of the system, of the methadone treatment providers and probation officers. Steven was among the many people I encountered who had initially started using legally obtained opiates to treat pain from work-related injuries, only to find their access limited by increasingly stringent state prescribing regulations. People like Steven turned to heroin not because they preferred it, but because they could no longer get prescription painkillers.Conversations with addiction medicine providers echo the judgment about which some of the drug users I’ve spoken with complain. In the <em>New York Times’</em> coverage of the suburban opiate panic, doctors identify with their patients, perhaps even knowing them socially. This is not the case in Vermont, where the class divide between doctors and patients is wide. Even the most sympathetic physicians I spoke with endorsed monitoring and coerced treatment. One said that there was “no high-level thinking in Vermont” and “no one understands the medical piece.” When I asked about the best way to treat addiction, this doctor told me it was suboxone (buprenorphine) combined with “tight control… put an ankle bracelet on them and tightly monitor them… If you mess up, you go to jail. Folks do best when there are consequences.” Other medical providers were frustrated with their patients, viewing their poverty-related struggles such as lack of transportation or difficulty finding employment as “excuses” for not succeeding in recovery. Their patients’ continued smoking and poor eating habits are also a regular source of frustration. One doctor who called addiction a “disease” insists that the criminal justice oversight of a sick person is not a contradiction, but a mechanism to ensure sorely needed “accountability.”In my book <em>Judging Addicts</em>, I detailed the merger of the medical and punitive frameworks of addiction and how they’ve come to characterize the modern treatment system in the U.S.: criminalization and medicalization are complementary, rather than contradictory approaches, I argued. This merger is apparent in Vermont where the treatment and punishment systems are deeply intertwined. And yet, this mingling has not necessarily led law enforcement to a more progressive or lenient view of addicts or for medical providers to argue that addicts shouldn’t be criminally punished. A prosecutor who was assigned to a drug court told me: “Their problem isn’t really addiction, their problem is that they’re criminals. And their parents were criminals.” This person was reluctant to accept the narrative that these people were sick even though she was working as part of a Drug Court Team whose ostensible goal was to get addicts the services they need to become drug and alcohol, and thus crime, free.<dl id="attachment_7516" class="wp-caption aligncenter" style="width: 680px;" data-mce-style="width: 680px;"><dt class="wp-caption-dt"><a href="https://contexts.org/files/2017/12/20626846824_18ad3414a4_k.jpg" data-mce-href="https://contexts.org/files/2017/12/20626846824_18ad3414a4_k.jpg"><img class="size-large wp-image-7516" src="https://contexts.org/files/2017/12/20626846824_18ad3414a4_k-680x453.jpg" alt="" width="680" height="453" data-mce-src="https://contexts.org/files/2017/12/20626846824_18ad3414a4_k-680x453.jpg" /></a></dt><dd class="wp-caption-dd">U.S. Marshals and police undertake Operation "Salt City" in Syracuse, New York, 2015. The actions led to 248 arrests and the seizure of cash, firearms, and drugs including heroin. <a href="https://flic.kr/p/xqHYW5" data-mce-href="https://flic.kr/p/xqHYW5">Shane T. McCoy/US Marshals</a></dd></dl>Policing FamiliesAddiction becomes the pretext for a system of punitive social control over people whose long-standing poverty has made them objects of particular scorn. And it’s not just the medical and criminal justice systems. The Department of Children and Families is equally involved in many people’s lives. The head of DCF attributed the recent 40% increase in cases of children removed from their homes and placed in state custody to opiate addiction, despite data that indicates no statistically significant increase in opiate use in the state over the past decade. Children are being removed from their parents at such high rates that the Defender General had to hire several new attorneys just to handle these cases. Defense attorneys talked about the new “zero-tolerance” policies toward opiate-using mothers, how child protection staff and judges believe the opiate users they encounter are unfit parents solely because of their drug use. Once children are removed, parents face considerable obstacles in regaining custody. The combined conditions of stable housing, full-time employment, clean urinalysis, and regular attendance at drug counseling sessions (sometimes several a week), often without a car, prove insurmountable for many.Through my years of research, I have observed a social control system of poor White drug users that resembles many of the findings in studies of poor addicts of color in urban areas. The experiences of poor White drug users in rural Vermont reveal the same “hostile exercise in disciplining” that anthropologist Phillipe Bourgois observed in his research among low-income African-American and Latino methadone patients in New York City and San Francisco. Their addictions were “disciplined” through a quasi-punitive and medical treatment model in much the same way the addictions of many White drug users in Vermont are.<dl id="attachment_7517" class="wp-caption aligncenter" style="width: 300px;" data-mce-style="width: 300px;"><dt class="wp-caption-dt"><a href="https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388.jpg" data-mce-href="https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388.jpg"><img class="size-medium wp-image-7517" src="https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388-300x270.jpg" alt="" width="300" height="270" data-mce-src="https://contexts.org/files/2017/12/17673953779_82dc0ade4d_k-e1513518685388-300x270.jpg" /></a></dt><dd class="wp-caption-dd">A woman holds up a photo of her son at a "Heroin Summit" with the Lt. Governor of Maryland. <a href="https://flic.kr/p/sVMCH2" data-mce-href="https://flic.kr/p/sVMCH2">Joe Andrucyk, MarylandGovPics, Flickr CC</a></dd></dl>Expanding PunishmentMany of the people I’ve spoken with have had long-standing involvement with the criminal justice system. The enhanced cooperation among treatment and criminal justice has been strengthened because of the attention the opiate panic has received. This increased attention, in contrast to reports from suburban White America, has been accompanied by heightened policing. In June 2017, the Vera Institute of Justice released a report titled <em>Out of Sight: The Growth of Jails in Rural America</em>. It showed that the use of jails in rural areas has dramatically increased as it has declined in urban areas and asserted that this “new rurality of jails” is led, in part, by the growing incarceration of White people. Between 2004 and 2014, the percentage of White people in jail grew 19% in rural counties and 15% in small- and medium-sized cities. The <em>New York Times</em> has identified Dearborn County, Indiana as one of the most punitive places in the U.S. Over 97% of its inhabitants are White.While violent crimes drive state and federal prison admissions, drug arrests and property crimes largely fuel the increase in admission to local rural jails. The criminal justice system does not collect information about social class, greatly limiting our ability to quantify the extent to which poverty plays a role in policing, prosecution, and sentencing decisions. But, from my research in Vermont and conversations with actors involved in the criminal justice system, I have seen how the mechanisms of social control deployed against poor White opiate users rely heavily on criminalization and look nothing like the “gentle” narrative portrayed in national media.Jeff Sessions, currently the nation’s Attorney General, has made his intention clear: he will “aggressively prosecute” drug crimes. He has used the opiate crisis in his justification for no-tolerance policies. Local drug enforcement is not directly affected by federal policies but, given the rising rates of incarceration in rural America, there is little reason to doubt that county law enforcement will continue to jail its inhabitants, many of them White, at increasing rates. Political scientist Marie Gottschalk, in <em>Caught</em>, has argued that prisons are “resilient institutions” able to absorb critiques and emerge stronger. She points to arguments about racial bias, showing how some states simply increased their custodial control of White people to “equalize” incarceration rates between Whites and African Americans.There are reasons to expect that White opiate users would receive better treatment than Black drug users, and much of the media rhetoric bolsters this assumption. But rhetoric is not reality in rural America. From New England to Appalachia, officials’ approaches to fighting opiates have largely involved a criminal justice response. Nor is the heightened punitive control of poor rural Whites new: The “meth panic” of the 1990s was accompanied by the criminalization of drug users, many White, in places like the Midwest. Again, the assumption that all White drug users are receiving better treatment because they are White ignores the stark class difference between suburban and rural drug users and the decades-long criminalized control of the latter. Poor White drug users complicate the dichotomies that characterize contemporary drug abuse discourse: poor and minority versus middle-class and White, prison versus treatment, addiction versus depravity.It would appear that the long-standing poverty of many drug users in Vermont is itself being criminalized. As the superintendent of a local jail told me, most of the inmates are poor and they often need to come to jail to get stable housing and regular meals. “It’s sad,” he said, shaking his head, “it shouldn’t be this way.”The national hand-wringing over opiates highlights the middle-class at a time when poor rural Whites are one of the fastest growing populations under criminal justice supervision. The media-framed drug panic obscures this inequality and exacerbates racial tension about the War on Drugs by focusing on the addictive drug that unites White opiate users rather than the class differences and inequality that divide them. As the criminal justice system modifies to withstand criticism, so too must those of us who care about drug policy and the effects of criminalization. Panic should not inform policy or displace the fact that criminalization reinforces class and race distinctions to the detriment of entire communities.Recommended ReadingsCaroline Acker. 2001. <em>Creating the American Junkie: Addiction Research in the Classic Era of Narcotic Control.</em> Baltimore, MD: Johns Hopkins University Press. A highly readable history of the first major U.S. opiate scare and the way in which medicine, psychiatry, and law combined to create the “junkie” figure so prominent in our cultural imagination.Jason Cherkis. 2015. “Dying To Be Free,” <em>Huffington Post</em>, January 28. A multimedia essay illustrating the moral discourse that prevents heroin users from getting humane and life-saving treatment.Marie Gottschalk. 2015. <em>Caught: The Prison State and the Lockdown of American Politics.</em> Oxford, UK: Oxford University Press. Gottschalk presents meticulously analyzed data about punishment trends, including those that affect poor rural Whites, to argue that reforms based on racial inequality or race neutrality will fail to address the prison state’s expansion.Helena Hansen and Jules Netherland. 2017. “White Opioids: Pharmaceutical Race and the War on Drugs that Wasn’t,” <em>Biosocieities</em> 12(2). The authors argue that because the opiate panic is a “White drug war”, it’s characterized by a less punitive, more clinical approach than is customary of drug panics focused on people of color.Craig Reinarman. 1994. “The Social Construction of Drug Scares,” in Peter Adler and Patricia Adler (eds), <em>Constructions of Deviance</em>. Belmont, CA: Wadsworth Publishing. A modern classic, this analysis of drug scares outlines their seven main ingredients and demonstrates that drug panics obscure the underlying racial and class tensions that precede them.